Calculation of Systemic Score
Clinical manifestations of MFS in other organ systems were critically evaluated for their specificity and diagnostic utility based on expert opinion and the available literature. Several of the “minor” criteria from the old Ghent nosology were eliminated, but the most selective systemic features were included in the “systemic score”.
Systemic Score
To learn more about each physical characteristic, click on the accordion links below:
-
1. Wrist and/or thumb sign
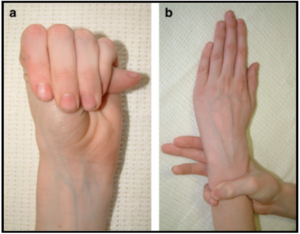
The thumb sign is positive when the entire distal phalanx of the adducted thumb extends beyond the ulnar border of the palm with or without the assistance of the patient or examiner to achieve maximal adduction. The wrist sign is positive when the tip of the thumb covers the entire fingernail of the fifth finger when wrapped around the contralateral wrist.
-
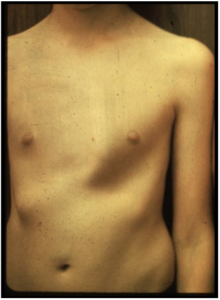
2. Anterior chest wall deformity
Pectus carinatum is believed to be more specific for MFS than pectus excavatum and is assigned two points. Subjective qualifiers in the original Ghent criteria such as “requiring surgery” have been eliminated but the examiner should be confident that a positive finding (pectus excavatum or chest wall asymmetry) extends beyond normal variation of chest contour in the general population before assigning one point.
-
3. Hindfoot deformity
Hindfoot valgus in combination with forefoot abduction and lowering of the midfoot (previously referred to as medial rotation of the medial malleolus) should be evaluated from anterior and posterior view. The examiner should distinguish this from the more common “flat foot” (one point) without significant hindfoot valgus.

-
4. pneumothorax
Any spontaneously-occurring pneumothorax
-
5. Dural ectasia
For the detection of lumbosacral dural ectasia, no preferred method (CT or MRI) or uniformly accepted cut-offs have emerged from the literature and local standards should apply.
-
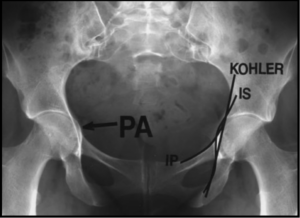
6. protrusio acetabulae
On X-ray anterior-posterior pelvis angle, the medial protrusion of the acetabulum above 3 mm beyond the ilio-ischial (Kohler) line is diagnostic. Criteria on CT or MRI are not precisely defined but involve loss of the normal oval shape of the pelvic inlet at the level of the acetabulum.
-
7. Reduced US/LS and increased armspan/height ratio
The combined presence of reduced upper to lower segment ratio (for white adults <0.85; <0.78 in black adults; no data have been assessed in Asians) and increased armspan to height ratio (for adults >1.05) in the absence of significant scoliosis. Please add one point to the your score if the systematic score is positive. In Asians the incidence of an enlarged armspan to height ratio in Marfan patients was noted to be lower (25) and prior studies of Asian (and also Afro-Caribean) populations demonstrated different distributions of armspan and height, so one should consider these ethnic differences when using cut-off values (26). For the US/LS ratio in children, abnormal ratios are US/LS < 1 (for age 0-5 yrs), US/LS < 0.95 (for 6-7 yrs), US/LS < 0.9 (8-9 yrs old) and < 0.85 (above age 10 yrs). The lower segment is defined as the distance from the top of the symphysis pubis to the floor in the standing position and the upper segment is the height minus the lower segment. Importantly, neither of these ratios provides an accurate measurement of bone overgrowth in the presence of severe scoliosis or kyphosis.
-
8. Scoliosis or thoracolumbar kyphosis
Scoliosis can be diagnosed either clinically if, upon bending forward, a vertical difference of least 1.5 cm between the ribs of the left and right hemithorax is observed or if a Cobb’s angle (angle between a line drawn along the superior end plate of the superior end vertebra and a second line drawn along the inferior end plate of the inferior end vertebra of the scoliosis measured on anterior-posterior view of the spine) of at least 20° is seen on radiographs. In the absence of scoliosis, one point can be contributed by the presence of an exaggerated thoracolumbar kyphosis.
-
9. Reduced elbow extension
Elbow extension is considered reduced if the angle between the upper and lower arm measures 170 degrees or less upon full extension.
-
10. Three of five facial features
One point can be assigned based upon facial characteristics if the patient shows at least three of the five typical facial characteristics including dolichocephaly, downward slanting palpebral fissures, enophthalmos, retrognathia and malar hypoplasia.
-
11. Skin Striae
Striae atrophicae are considered significant as a diagnostic feature if they are not associated with marked weight changes (or pregnancy) and if they have an uncommon location such as the mid-back, lumbar region, the upper arm, axillary region or thigh.
-
12. Myopia
Given that myopia is very common in MFS, is routinely monitored, and tends to show early onset, high severity and rapid progression, myopia of greater than 3 diopters contributes to the systemic score for diagnosis. However, since myopia is quite common finding in the general population we have only attributed one point to it in the systemic score.
-
13. Mitral valve prolapse
Mitral valve prolapse should be defined by echocardiography as protrusion of one or both of the mitral valve leaflets across the plane of the mitral annulus during systole. This is best detected in parasternal long-axis or apical long-axis 3-chamber or 2-chamber views. There are no special criteria for diagnosing MVP in MFS and standard practices should be applied.